Here is my training video with Dr. Alan Hopkins where we share our newest resource with you: Self-Order Labs (urine, blood, and DUTCH). No more begging or negotiating with your doctor. You can now order the labs yourself.
What you will learn from this interview:
- Introduction to Dr. Alan Hopkins and a brief overview of his professional credentials
- Basic fundamentals you need to know about direct access lab testing
- The importance of proper nutrition and testing for nutritional deficiencies
- Thyroid testing and the different ways it’s done
- The latest technology to evaluate cholesterol
- Inflammation and hormonal balance
- Lab Panels offer for the Hormone Balance community
(This interview was recorded in October 2018)

Magdalena W.: Hey, you guys, this is Magdalena here, Hormones Balance. I’m here today with Dr. Alan Hopkins. I’m super excited to be able to bring to you a way to order labs, urine as well as blood on your own without having to negotiate, argue, and beg a doctor for ordering these labs which so many of you are asking us every day what should I order, how should I order?
This, it took me a while to figure this part out because I couldn’t do it on my own but then there are, obviously, people that are creating these opportunities for us. Today, what we’re going to be discussing with Dr. Alan is, what are the markers that are really important in hormonal balance? I think that’s the first thing we’re going to be looking at because it’s not just hormones. What you’re going to discover today is not just hormones that we want to measure, we also want to measure a lot of other imbalances that are happening in the body that actually cause hormonal imbalances. Many of you have asked us about DUTCH, that’s one of my favorite urine testing panels and so we’re going to be talking about that as well because we found a way to actually order the labs from them directly through Dr. Alan and his company.
Alan Hopkins: Yeah, hey, super excited and really excited to be here to talk to your community about direct access lab testing and in this particular resource. I think it’s awesome and I’m super excited to get started. I did prepare a PowerPoint for you, guys, that I’ll be happy to share as well
>> Click here to download the presentation SLIDES
Magdalena W.: Awesome. Before we transition over to the slides showing you what to order, what do the different markers mean, which I think is a wonderful educational piece? Towards the end, we’re going to be talking about the different panels that we created for the hormone imbalance community so there’s going to be three options and two of them include DUTCH as well.
Also, the good news is that if you are a health coach and you work with clients, you might find this presentation incredibly powerful as well and super helpful. In fact, Dr. Alan, I think a lot of your clients right now are health coaches, right, because it really empowers them on how do you work with patients so with clients and how do you help them through their nutritional deficiencies and imbalances.
Alan Hopkins: Yeah, absolutely. I mean we’ve made a business decision to work closely with health coaches to try to provide them value in their own practice. Health coaches are typically those people who have had some issues in their life or they’re just optimizers where they just want to be as healthy as possible and they’re yearning for education. It’s not only direct access lab testing, but it’s also what do these tests mean, what is considered normal values and then what are the optimal values. It may be functional medicine doctors or anti-aging doctors would want to see you at, and so I do want to talk a little bit about the differences but yes, in general, health coaches are fantastic people to work with and a lot of health coaches love this platform.
Magdalena W.: Yeah, okay, awesome. I think we are ready for the slides.
Alan Hopkins: Okay, all right. Well, cool. Let’s see if I can share them. All right, so can everybody see those okay? All right, so I want to talk about using biomarkers to prevent premature aging and how it’s relevant to hormones, and Magdalena, can you see the PowerPoint?
Magdalena W.: I can but I think you need to project it as a presentation.
Alan Hopkins: Okay, let me just start it from … How about there, is that better?
Magdalena W.: Perfect.
Dr. Alan Hopkins Background
Alan Hopkins: Okay, perfect. Before I start though I want to tell you a little bit about myself so you know who’s talking to you. I currently work as a professor at the University of Texas at Austin in the Dell Medical School, a fairly knew medical school by the way. I am a medical doctor with an MD degree from one of the blue zones.
If you’ve ever heard about the five blue zones in the world, Loma Linda is actually a blue zone. It’s where they have more people who live longer than 100 years in the world. From that, I sort of learned a lot. What I loved about Loma Linda is it was a very whole person approach to health care. In other words, it wasn’t John with colon cancer in Room 18. It was, “Hey, you know, here’s John. He’s married. He has three kids. He works as a computer analyst and unfortunately, he’s been given the diagnosis of colon cancer, how can we best help him?”
It was a very well-rounded educational opportunity that I had there at Loma Linda and I really appreciated it. However, I went into emergency medicine and as a board-certified emergency medicine doctor, I found my life to be somewhat frustrated because in the last 20 years I have literally seen more cancer than I’ve ever seen before, diagnosed far more cancer, more obesity which more diabetes, earlier strokes and heart attacks than I’ve seen at the start of my career so I began to ask myself the question, “What is going on out there? Really, why are we having trouble with so much chronic disease and what are we doing in medicine to actually help?” Because it just seems like, what we’re doing, whatever it is, it’s simply not working.
From that, I did some advanced training with A4M which is about 25,000 practitioners from all over the world in all sorts of different specialties that have been somewhat disappointed with conventional medicine. In fact, there’s a lot of conventional medicine people who are just looking for other resources and other things to help their patients.
Here’s a good example, nutrition. I only got a couple of hours of nutrition education in medical school and proper ways of eating are probably one of the best ways to actually help people and doctors are given very little training on this. The idea was that maybe we could learn something. A story came to mind of a neurosurgeon who had people with inoperable brain tumors and he was there saying, “Look, I’m a great surgeon. I would love to take out this brain tumor but I just simply can’t take it out because of its location in the brain. I’ll kill the person.” He would try people on diets and he was trying the ketogenic diet and he was showing us that for a certain subset of cancer patients on this ketogenic diet he could actually shrink the tumor just from dietary intervention alone. But that just gives you an idea that there are people out there that are looking for more well-rounded approaches.
Now, having done this additional training, I got hired to be a consultant for a company called Biophysical Corporation. They did advanced biomarker testing or lab testing for shows like NBC’s Biggest Loser, you might have heard of that. They did The Oprah Show and Oprah Winfrey herself went through her biophysical lab protocols and so I had a great opportunity to really learn a lot in a much deeper way about advanced biomarker testing.
From that, I became a medical director for PHDx which is an advanced diagnostic company here in Austin and I ultimately formed my own company for consumers and it’s a direct access lab testing company for the public called YourLabWork.com. I did that because I had people who had tremendous increases in their deductibles, they were forced to pay cash for things and unfortunately, that’s how medicine has gone these days.
If you can see that … This is from the New England Journal of Medicine, so these are my people, conventional medicine. This article’s from earlier this year, it was written by two doctors that are arguing about trying to do away with the annual physical. They think it’s a waste of money. They think preventative lab testing is a huge waste of money and they’re trying to encourage us to just get rid of it. Well, I don’t know if you’re like me but when I grew up into my early adult years, that time during the annual physical was a time to really get to know my provider to form a relationship for them to get to know my family and my concerns, not only about my health but maybe what was going on with my job and my stress, my sleeping patterns, these kind of things that are so important in health. It was also a time for them to run preventative medicine labs and then to do interventions or screening tests.
The whole idea here is that they’re really doing away with this. Doctors these days have very limited time. They have just a few minutes with people and they’re looking for disease so they’re making a diagnosis, they’re writing a prescription and they’re sending you out the door. A lot of times people feel like they’ve been shortchanged in their office visit for this and there’s been tremendous frustration. Nowadays people are taking matters into their own hands and they’re wanting to know more and learn more. Fortunately, with all the online information, there’s plenty of information for people to research.
As a company, we wanted to be a company that was able to provide solid research-led education to people and so we put together some objectives that we want to talk about today. We want to talk about some basic fundamentals you need to know about direct access lab testing. We also want to talk about the basics of hormones, on how to get proper testing done because hormones are so important. But like you alluded to at the very beginning of this, without proper nutrients, we have improper metabolism and we can have trouble actually making hormones.
We also want to talk about thyroid testing and the different ways that it’s done. I’m going to show you a couple of examples and then I’m going to also show you the latest in technology to evaluate cholesterol, which I think is really interesting. Then finally we’re going to talk a lot about inflammation. This is the real up and coming thing. People are really learning that inflammation is at the root of most chronic diseases so there’s huge impact there. Then finally, we’re going to talk about how insulin can really impact weight loss and can really predict future disease and it’s important for you to know if you’re at risk. Then finally, we have the special offer for this community, this hormones imbalance community that we’re going to present to you for your consideration.
All right, so I want to talk about aging well and we’re going to talk a lot about hormones but hormones are just one piece of the overall pie when it comes to health. This is an aging well circle and I wanted to just point out in the middle of this circle are the non-modifiable risk factors. We haven’t figured out a way to actually stop chronological age, people are just getting older. They’re born a certain gender, they’re given a certain genetics and they’re of a certain race, and these are the things that are considered to be non-modifiable.
Outside of this circle, however, are all the things that can be fixed, if you will. Many of you are familiar with the top one there, the vascular integrity, that one there has to do with cholesterol. Now, I can tell you as a doctor that in the 1970s, we were very convinced that cholesterol was killing people and that we had to do everything we could to get rid of cholesterol from dietary intake and so the big fads of non-fat and low fat and so on all originated from that. Unfortunately, everything there got replaced with sugar and so now we’re seeing an epidemic of diabetes and prediabetes and so on. If you look at the circle down to the right, it says insulin dynamics. This really talks about do we have any sugar issues? Do we have something called insulin resistance syndrome which is the first sign of going on the road to diabetes? Or maybe we have prediabetes already? Ninety percent of people with prediabetes don’t know they have prediabetes and 90% of people with prediabetes don’t have any symptoms so how would they know unless they get checked.
Then to the left, there is something this community is very familiar with, it’s hormones, not only the sex hormones but there’s also thyroid hormones that could be checked and then stress hormone, cortisol. Cortisol is a test, a great example of a test that I find very helpful to get a blood test first thing in the morning when you wake up because if it’s super low then I try to encourage people to get their sleep evaluated in a formal way because many people have undiagnosed sleep apnea and I’ll tell you this. If a person gets their sleep apnea properly diagnosed and treated, it can improve cholesterol numbers, it can reverse diabetes and prediabetes. It can also give them more energy than they’ve had before and it brings the adrenal gland back into better function and can improve the overall function of all their hormones.
Then finally, nutrition, we can also measure these with blood test too, looking at B levels, B12, and folate which is vitamin B9. Many women are deficient in serum ferritin which is a transport protein for iron and then, of course, magnesium, a very common deficiency. If we’re looking at an overall aging well wheel here, we have to approach people in a very comprehensive way. Just like I was trained at Loma Linda that the person is not the disease, a person is a person and we really have to take a very comprehensive look at their life in order to actually let them age extremely well.
The outer part of the circle deals with this. We talk about sleep, making sure that people are sleeping well, sleeping long enough, don’t have obstructive sleep apnea and feel great after sleeping. Stress, so important to address, to understand people’s stress points whether it’s their family or their job or so on. If this is not addressed, this can cause problems. Smoking, of course, it’s pretty obvious nowadays but smoking increases your risk by threefold for stroke and heart attack so it needs to be stopped.
Allergies, this is something that keeps people awake at night and interferes with sleep so that needs to be addressed as well. Nutrition, this one’s probably the most obvious. There’s so many books and so many fad diets out there, whether you’re a keto or a paleo or a plant-based or whatever, there’s a nutrition intervention for everyone. Social dynamics, this has to do with really understanding where a person is coming from and what their triggers are. How are they going to be supported? I mean we have many people that we want to put them on a certain diet but it doesn’t work for their family because they’re the primary caregiver, they cook all the meals and their family is not going to tolerate it. Well, we have to consider that.
Then of course if you’re overweight, many people want to lose weight and the side effect of properly understanding your lab tests are oftentimes the side effect is weight loss. Physical activity, of course, the more you use your body, the longer you’re going to live and be active. Then if you ignore all this stuff, to the right is everything that I see more of in the last 20 years in the ER. Earlier strokes and heart attacks, blood pressure problems, cancers, autoimmune disease, leaky gut and so on. You can see that if properly screened for and addressed, a person can truly age well.
Hormones and Proper Testing
Now, I want to talk a little bit about hormones and proper testing. There are various ways, and many of you are familiar with this, of measuring hormones. We can do blood testing. We can test hormones in the urine such as the DUTCH test or we can do swab test or salivary testing for hormones. My personal opinion is that there are some ways that are preferred so I really like to check insulin with a blood test. I like to check thyroid hormones with a blood test and also, I don’t know if you know this or not, but your fat actually is the largest endocrine organ in your body. Your belly fat, also called visceral fat, makes either hormones that are pro-inflammatory leading to inflammation or they make hormones that are protective for you, anti-inflammatory hormones and these can be measured through a blood test.
Female hormones, these can be measured through blood test and also urine test. The DUTCH complete testing is something we just started offering. Also, adrenal hormones, what about them? Well, I talked a little bit about how I measure the AM cortisol with blood work and if it’s inappropriately low, it makes me suspect obstructive sleep apnea and we make sure that the person doesn’t have that because if they do have it and we treat it, it fixes so many things.
You can also measure patterns of the way that your hormones are being secreted and these patterns can be measured with DUTCH testing or salivary testing. All right, so the DUTCH complete. This is an example of a test that can be shipped to you. It’s shipped to your home and you, basically four or five times during the day, you provide a urine specimen and you let it dry on this little piece of paper and then you send it back into the company. This gives a complete assessment of the sex hormones and also a comprehensive assessment of what that cortisol or adrenal hormone is doing throughout the day along with some of the metabolites from the adrenal gland.
It really is designed to be optimally effective for most forms of hormone replacement therapy so it is a test that it’s very comprehensive and it’s a fantastic snapshot of where your hormones are at. By the way, it can also measure some neurotransmitter metabolites, things that work with your brain.
Magdalena W.: Sorry, can we just go back to the previous slide.
Alan Hopkins: Sure.
Magdalena W.: I just want to mention because not everybody knows, the sex hormones will include things like DHEA, testosterone, progesterone, estrogen. I don’t think they measure pregnanolone, they don’t, unless it’s something in you. As you said also, the adrenal hormones will be cortisol here. I just want to make sure that everybody understands it’s a very comprehensive panel.
The DUTCH really looks into metabolites which is how the hormones get broken down and there’s various aspects including nutritional deficiencies, including stress, including inflammation, that can impact how the hormones are broken down. A good example is estrogen. Dr. Alan, one of the things that has been a struggle, an ongoing education on my part is that women are so afraid of estrogen because of estrogen dominance, right, but yet, we wouldn’t function as women, we wouldn’t have boobs, periods, juicy vaginas without it, right, and strong bones.
Yet, the question is how we break down those estrogens and that’s exactly what DUTCH shows and that’s why I am a big fan of this test, of this panel.
Alan Hopkins: Yeah, I absolutely agree with all of that. There are about 400 protective effects of estrogen in the body and without estrogen, we start to have a lot of problems and we certainly are … we’re going to talk about some of those things that may not be obvious to you guys that will happen if you don’t have the proper amount of estrogen.
DUTCH, what I like about it, in assessing it, is it gives so much data and of course, doctors love data. Patients if they understand it really love data too and really, this is what lab testing is all about is it’s giving us our own individual data that we can then act on and so our job for you is to provide you the resources that allow you to act on this in the most effective way.
Magdalena W.: Now, here’s a little catch with DUTCH. Because of its complexity, it’s not designed for an end user, for a patient to look at this and go like, “Oh, I know exactly what’s going on and what I should do.” It really is the practitioner needs to be trained on this so the good news is we’re going to talk about this towards the end. We have partnered up with a doctor who does telemedicine and can help you with interpreting DUTCH results once you get the results.
Alan Hopkins: Yeah, absolutely. Yeah. He’s an OB-GYN that specializes in this DUTCH testing and so, we’re going to talk a little bit more about that at the end but DUTCH complete is a new offering for us we’re really excited about.
Now when it comes to hormones, we also have to look at other things, right, so we’re going to look at some of the common nutrient deficiencies here just for a minute and we’re going to talk about how they’re relevant to hormones.
Nutrient Deficiencies
Well, first of all, I don’t know if you guys knew this or not but about 90% of Americans are deficient in the amount of omega-3s that they have. It turns out that omega-3s can protect you from osteoporosis as you get older and this is because omega-3s help suppress inflammation. We know that chronic inflammation will disturb the bone metabolism. Omega-3s do so many wonderful things in addition to lowering inflammation. They can increase our HDL cholesterol which is our good cholesterol. They can decrease triglycerides.
In fact, we find that the more omegas you take, either in your diet or you take as a supplement, the lower your triglycerides will go. Omega-3s can also lower this amino acid. It’s an advanced biomarker called homocysteine. If you have high homocysteine levels, you’re at a higher risk of cognitive decline and Alzheimer’s. Very strong association between high homocysteine and Alzheimer’s, Alzheimer’s in any form of cognitive decline.
There’s also something called lipoprotein A which I’m going to teach you about in a minute that I think it’s so important for everybody to know whether or not they have lipoprotein A. It’s a genetic factor that really increases your risk for heart disease but omega-3s can actually lower lipoprotein A so it’s important to know that. Omega-3s also tend to shift the person from the small dense dangerous cholesterol to the lower more lightly fluffy kind. We call the light fluffy kind pattern A, and omega-3s can help you get there. There’s a lot of really great advantages to omega-3 and as you can see 90% of people are deficient so very likely in your testing, you may not be optimal.
The same goes with vitamin D, and I think this is probably something that’s probably a little more well-known now and the reason why is because we see so many benefits to vitamin D. If you want to talk about it in terms of its relevance to hormones, it’s very strong bone builder and it protects you from osteoporosis as you age. We also see really good data around less cancer risk for many different types of cancer, better control of blood pressure, less depression.
It can increase your HDL cholesterol and we think that it helps the insulin actually work better, make it more efficient. We’re giving it to people who have seizures and we’re finding that if they’re at higher levels of vitamin D, they tend to have less seizure problems. Same thing if they have psychiatric disorders, if they have a psychiatric disorder and we optimize their vitamin D, we see less of their breakthrough psychiatric issues so it is really important, vitamin D. It’s more of a hormone than it is a vitamin.
Magdalena W.: Yeah. Just it reminds me too on vitamin D, adequate level of vitamin D is also important in conversion of T4 to T3 hormone, right?
Alan Hopkins: Yes.
Magdalena W.: I can’t tell you how many women has started supplementing with vitamin D, especially like the one that we have is the D3 with K1 and K2 and the hair growth has come back within a couple of months. Just really … Because what we were talking about right at the beginning that hormones really to me is always the last point that goes out of whack because of the other imbalances that happen in the body, right?
Those nutritional deficiencies you’re talking about because of the stress, because of the lack of sleep, whether it’s apnea or other reasons, so so important to address this is an underlying reason.
Alan Hopkins: Absolutely, yeah, that’s a great point. Yeah, such a great point. When it comes to hormones like everything else, it requires a really comprehensive look from a bird’s eye view on a person’s total health in order to get your hormones optimized.
Magnesium, another common thing that people are deficient in, and many people have trouble with falling asleep and sleeping well and magnesium can help with that. We also see less depression, less fatigue, blood pressure control.
Magnesium does this because it relaxes the smooth muscle cells in our body so we certainly see this in asthma in the emergency room. If someone comes in in acute distress, [inaudible] because their asthma is so out of control, we’ll give them IV magnesium and it relaxes the smooth muscle cells or the breathing tubes and helps open up those breathing tubes so they can exchange air, so magnesium is very important. Again, it’s not something that we’re seeing people at optimal levels very often.
There are all kinds in addition to the omegas and the vitamin D and the magnesium that we want to look at. We also want to look at, for example, serum ferritin. This is the transport protein for iron that I mentioned before. Many women are very low in their serum ferritin levels and serum ferritin levels less than 41, you need to replace that, that iron in your diet or through a supplementation. B12 and folate are also very common, people are deficient in those. That can lead to higher homocysteine levels which I’ve talked about being a marker for cognitive decline, at least a risk factor for cognitive decline.
We’ve done studies, we’ve looked at people with Alzheimer’s who had higher homocysteine levels and we said, “Hey, you know what, if we give these people B12 and folate and we watch them over time, will it slow down their Alzheimer’s?” Well, we found out that it doesn’t. Now we’ve gone to the question of, what if we knew about this 10 or 15 or 20 years before the Alzheimer’s diagnosis and we treated it? The consensus out there in the community is absolutely treated high homocysteine levels or people that are deficient in B9 which is serum folate and B12 because they make up this thing called the methylation pathway.
Again, these things are very commonly a problem, these nutrient deficiencies that we talk about. The other things that can be measured, we’ve talked a little bit about and we touched about them, and now I’m going to go into very specific examples for you guys on this aging well panel on how we can look at some specific examples, so let’s talk about thyroid. You mentioned the thyroid and how vitamin D does help with the conversion of T4 into T3. I just want to give an overview.
Thryoid Overview
Thyroid disease is especially common among women. For every man that has a thyroid problem, about 9 or 10 women have a thyroid problem. This is very much linked to women and there’re several reasons why. But if you’re a woman and you haven’t had your thyroid checked in the proper way my argument is that you should get it checked in the proper way and you should get a fairly complete thyroid assessment.
Your brain produces something called TSH or thyroid stimulating hormone and it tells your thyroid, which is butterfly shaped gland in your neck, to produce these thyroid hormones, they’re T4 and T3. T4 is inactive, 80% of which your thyroid makes is inactive thyroid hormone. You may say, “Whoa, why is my thyroid making mainly inactive hormone?” or, “Why wouldn’t it make active hormone?” Well, this is the body’s flexibility. When you do this, it allows your body to convert T4 into the active hormone which is T3 whenever it needs it. If it doesn’t need it, then it will store it as reverse T3, so it’s sort of the master regulator gland, the thyroid.
We produce stuff that we don’t use until we need it, and then about 20% of what the thyroid produces is the active thyroid hormone so we always have this basal amount of thyroid circulating around our body. When this goes awry, it can literally screw up every cell in your body, and this is one of the more undiagnosed conditions that we have. Here’s an example, somebody who came to our direct access platform and I’m just going to tell you their story and maybe you can relate to it.
This was-
Magdalena W.: Dr. Alan, sorry.
Alan Hopkins: Yes.
Magdalena W.: Before we dive in to the story, can I just suggest that let me just run through symptoms of low thyroid function because this is one of the most underdiagnosed and undiagnosed, misdiagnosed hormonal conditions, I think, right, with almost so many of us.
Alan Hopkins: Yeah, for sure.
Magdalena W.: Just quickly, because we get a lot of pushbacks from women saying, for example, somebody posts saying my hair is falling out and then we ask them, have you had your thyroid checked and they’ll say, “Yeah, my doc checked and everything is fine.” I’m really glad that you’re showing what to test for in a thyroid but I just want to remind our listeners that labs are labs and especially having a complete lab test is really important but you’re also going to couple that up with clearer symptoms, right?
Alan Hopkins: Oh, absolutely, yeah, so-
Magdalena W.: You are talking … Yeah, do you want to just run through the list of like typical symptoms for low thyroid patient because that’s the most common one?
Alan Hopkins: Yeah, absolutely, yeah. I would say definitely hair falling out it’s a big complaint. One of the bigger complaints we tend to get is weight gain. Although you can have a massive thyroid problem and not gain weight but weight gain is-
Magdalena W.: That was me.
Alan Hopkins: Yeah, weight gain is a big one. Then we also have depression, a huge thing. In fact, it makes me so upset when I see people put on antidepressants and they’ve never had their thyroid checked properly.
Magdalena W.: Yeah.
Alan Hopkins: We ultimately find out they have thyroid disease, what a waste and that person got labeled as something totally inappropriate. In addition to that though, thyroid disease can present in just about any symptom, that’s the problem with it, but in general we see the lack of energy which leads to people sometimes getting depressed or not having the same amount of energy, a lot of hair changes, nail changes, coarse skin, constipation, intolerance of cold, all of these things can be signs of thyroid disease.
Magdalena W.: Yeah. I will just add on to this also infertility. Women who have infertility issues, unfortunately, it’s so devastating. So many women lose their babies in the first three months, in the first trimester, without realizing that it’s a thyroid problem and never have that tested. That’s another, that could be another big one.
I also like how you said about the intolerance to cold. A typical thyroid patient will be that person walking around in the sweater in summer and always having cold hands and feet while everybody else is complaining how hot it is, right?
Alan Hopkins: Yeah, yeah, absolutely.
Magdalena W.: It’s your heat moderator. Like your pedal, it’s your speed pedal in every way. Brain fog, I would also add on to this because that’s something that I suffered from tremendously. Having anxiety attacks. That was also one of the things that I had, so yeah.
Alan Hopkins: Yeah. Thyroid is kind of like, it’s the great equalizer because so many symptoms it can present as and the problem is it doesn’t present with the same ones for every single person and so just like you mentioned you didn’t necessarily have the weight gain problem. There’s other people that do and that’s the challenge with thyroid disease and who do we test? Well, I mean if you’re a woman, you’re at very high risk and you should be checked.
I mean, I’ve gotten to the point now where I feel like a woman should monitor this every single year. They should get a thyroid testing done because it’s so common to have a thyroid problem. There’s about 29 million people out there with thyroid disease, most of them women. If you’re a woman and you haven’t had your thyroid checked, you really should be checked.
This story I wanted to tell you was about a lady whose name was Mary, very nice person, who had been to her doctor and been told her thyroid was fine and she had had a TSH done and she wanted to see if there was more extensive testing so she wrote us and said, “What other thyroid tests are there?” We told her, “Hey, this is a panel. This is how much it cost.” She’s like, “Oh, I want it.”
When it came back, I found it curious because I noticed here that suddenly she has a diagnosis. Now, if you’re a health coach out there or a non-provider, you really shouldn’t diagnose yourself but if you just sort of looked this stuff up and you have the proper education, then you know the question to ask that provider, is you say, “Do I have Hashimoto’s thyroid disease because these thyroid peroxidase antibodies are positive?” You can see that her free T3 and her T4 are at the lower end of normal but here’s somebody who had symptoms, who went to her doctor, who did a TSH, by the way, it was 4 at the time but that’s all they did, they just looked at the TSH.
Upon a more complete evaluation, there actually is a diagnosis here that needs to be acted on and this person here ended up going back to another doctor to get care. The idea here is that the information was out there, she was concerned, she had the resource, she ordered the test herself and that gave her the information she needed to go to somebody to get help, and that’s really what direct access testing is for. It’s for people to take on some of this information themselves and to act on it.
Latest technology to evaluate cholesterol
Some of the other things that we look at with advanced testing, getting back to your aging wheel here, is we’re going to look at cholesterol. I want to show you the difference really quick because I’m an ER doctor. So 50%, that’s five, zero, so 50% of people who come in with a heart attack are at their cholesterol goals. If they had a standard lipid panel which just looks at cholesterol and triglycerides and HDL and then does a calculation on the LDL, which is the lousy cholesterol, 50% of the people I see with heart attacks are okay.
What is going on? What are we missing here? Why are they getting heart disease? Well, it’s a combination of things but one of the latest tests that’s come out fairly recently has been this idea that it’s not just about cholesterol, it’s about the type of cholesterol that you have and more importantly than that, we understand that you can get subtypes of cholesterol.
If you go with me for a minute on this kind of busy slide, so at the bottom we’re looking at the diameter, in other words, how big these molecules are. Then on the Y axis or to the left is the density. That’s to the point of how much material they have packed inside. Is it super dense or is it more light and fluffy? Light and fluffy cholesterol markers are less problematic for us, and so if we have bad cholesterol, which is LDL cholesterol, we call it lousy cholesterol. If our lousy cholesterol molecules are light and fluffy we tend to get less heart attacks. We just do. However, if we have small and dense cholesterol that we tend to have the worst problems.
Then there’s a percentage of us, about 20% of us here in America that have this genetically modified LDL cholesterol molecule called LP little A or lipoprotein a. This is the smallest and most dense and most dangerous cholesterol marker you have. If you’ve ever seen anybody who’s really healthy, maybe you had a friend or a neighbor who maybe she went running and she had a heart attack and you’re like, “Wow, she was only 15 and she looked like she was in great shape.” That person may have had lipoprotein a.
I mentioned at the very beginning I worked with NBC’s Biggest Loser, and on that show, the trainer had a heart attack at the age of 50 and if you saw this, I think he was 51, if you saw this guy, you would notice, this guy is in extremely grate shape, amazing shape, but he had a heart attack due to the presence of high amount of lipoprotein a in his blood.
This is all online. You can Google it and find it about this guy, decent looking guy who had the heart attack and now he’s really speaking out about the importance of getting screened for LP little a. The problem is, and I fight with insurance companies all the time, is that insurance companies refuse to pay for this advanced cholesterol testing because they say, “Hey, why don’t you just put him on a statin? It doesn’t matter.” The problem is statins can actually increase LP little a. LP little a, I’m going to skip this for a second, just talk about-
Magdalena W.: Can I ask you a quick question on this? Is it genetic?
Alan Hopkins: Yes. This is genetic, this is genetic. This is extremely relative to women too by the way and the reason why is, if you’re premenopausal and you get your LP little a tested and it’s high, estrogen has a protective effect on keeping LP little a at bay. When you go through menopause and you lose estrogen, your LPA levels are going to climb and so that’s a strong argument for maybe in that person, maybe other risk factors need to be considered, but that person might be a good candidate for bioidentical hormone replacement therapy so-
Magdalena W.: So the LPA goes up, Dr. Alan, because estrogen goes down?
Alan Hopkins: Yes.
Magdalena W.: Okay.
Alan Hopkins: When estrogen goes away so when you’re postmenopausal and you can’t make any more estrogen you’re LPA levels will climb. I worry a lot about women who have LP little a and these are the women who die young and fit and in shape and it’s the 55-year-old women who you thought was everything fine and then she passed away in her sleep. There’s 1.2 million heart attacks in the United States every single year and about 120,000 of these are felt due to lipoprotein A. If you look for it you will find it and unfortunately, for me, I found it in my wife.
When I first heard about this and began reading about this I started testing everybody and I found it in my wife and because I knew it was genetic, I had her parents checked and I found it in her father, which made sense, and then at my work I found at one of my nurses who is super healthy, but I knew her mom had a heart attack at the age of 47 so we sent her in for some additional test, the calcium score, and we found a lesion in her coronary artery called the widow maker. It’s the left anterior descending artery of the heart. We found a lesion in the exact same place where her mother had had a stent put in when she was 48. We tested her mom and she also had very high levels of lipoprotein a.
The idea here is that if you have lipoprotein A, you need to know about it and there are certain things that can be done about it and we’re going to watch you much more closely than we would otherwise and it’s very important for us as consumers and people who care about our health to push this message out because right now insurance companies are trying to shut this whole idea down saying it doesn’t matter. We don’t need to talk about it. We don’t need to pay for it and so doctors don’t know a lot about it.
There are cardiologists that know some about it but we don’t really typically test for it until after the person’s had heart attack.
Magdalena W.: Yeah, this is really, really powerful. I mean I can think of two friends right off the bat who have history of parents having heart attacks at very young age with very healthy lifestyles, so this is really important and powerful. Needless to say, a lot of people in my community are like that, right? A question here for you, so what can a person like that do? I know that one of the things you will see in terms of the different packages that we have for you guys, education is an option there of exactly what do you do depending on the different markers, but just give me a little bit of a hope here even though this is genetic, what can, just very high level, what can a person do?
Alan Hopkins: Yeah, so there’s a ton that can be done when we know about it, right? I guess that’s my whole sermon here is to talk about how knowledge is power and just if you go to your provider and you say hey, I have LP little a, if they don’t know about it, it’s going to force them to read about it and learn about it.
If they don’t know about it, you might want to consider going to somebody else but a lot of my people will go and they’ll get early screening test done. There’s also intervention, some of them natural that need to be done. Here’s an example for you, particularly for women. If you have lipoprotein a, you’re much more likely to form a blood clot, I’m talking about a DVT or pulmonary embolus. For that type of a person I wouldn’t put them on birth control for that reason. Birth control increase your risk anyway so that and now you’re at a much higher risk because of your blood.
The other issue too is I would also consider testing postmenopausal so if you’re high premenopausal, I would test postmenopausal and consider at that point the possibility of bioidentical hormone therapy. Natural things that can be used to lower lipoprotein a, there’s numerous. You can try omega-3 fish oil. The problem is it only lowers it by about 10%. You can do niacin, the problem is 70% of people don’t tolerate it because it causes the flashing but we get the greatest movement with niacin. It will lower it by about 30%. There’s an online resource for people called the lipoproteinafoundation.org, and they have … and I recommend everybody go to that and I can give you the link for that but it’s a great way to actually … for people to realize how significant it is because it has the personal testimonies of people that were running in a race and they had their heart attack or stroke.
Anyway, and genetics, it’s really important for people to have their relatives checked, particularly if you’re in a high-risk family, in other words everybody dies kind of young from either a stroke or heart attack could be LP little a. I advocate for everybody to get checked and if you look at this pattern here. If you look at this worldwide map, we’ve always kind of thought, “Man, what are the Asians doing right? They’re eating more fish. They’re doing better, what’s going on here?”
Well, if you look at LP little a alone, their genetic prevalence is only 10%, the lowest of anywhere in the world. If you look at Africa, for example, their prevalence is the highest at 30%, and so there is this genetic difference between people but here in the United States, one in five people will have it and there seems to be an equivalency between male and female so being one gender or the other is not protective for you.
Magdalena W.: That’s incredible, that’s one in five, wow.
Alan Hopkins: Yeah. No, it’s super common and probably one of the most undiagnosed conditions that they’re out there. We’re talking today about a lot of things that are undiagnosed that now we can intercept disease instead of waiting for it. The only way you find out if you have lipoprotein a right now is if you’re proactive and you’re reading and you’re learning and willing to test for it. Otherwise, you’re going to have to wait till you have your stroke and heart attack and then the cardiologist might consider ordering it for you because maybe you look young and maybe you had your heart attack younger than expected but that’s how it’s getting done these days. It really needs to be diagnosed especially for women because they’re at a higher risk after menopause.
Just to touch on this. I know this is kind of busy but the idea here is that this is an advanced lipid panel so this is what I’m talking about is the technology that’s available out there right now. The first thing that I look at is lipoprotein a which is at the very bottom of this slide and this person here, super high risk. This is actually a physician who came through our platform, ordered his own test. When he got them back, he reached out to me and he was like, “Oh my god, what am I going to do? This lipoprotein a thing is super high.”
If you noticed lipoprotein a is a piece of the puzzle, the other is we want to know if he has high small dense markers. Remember I showed you that graph of what small dense things did. If you look at these LDL molecules from small to large you see LP little a is the smallest LDL molecule, right, so that’s genetic. You either have it or you don’t. If you get tested once and you’re normal, you don’t have to worry about that again but the LDL size still matters. If you’re low size, smaller, denser, that’s a person who’s higher risk. On his panel when we look at it, we look at does he have a lot of LDL smalls, so he also is at very high risk.
My point is a fasting lipid panel, it’s okay, but it totally missed his biggest risk factors were the fact that of his bad cholesterol, he had the worst kind and he also had genetically modified cholesterol that was the absolute worst kind so he-
Magdalena W.: Dr. Alan, I have a question for you on this one.
Alan Hopkins: He’s in big trouble.
Magdalena W.: Why is the HDL large a bad thing here?
Alan Hopkins: Okay, that’s a great question. HDL large is much better if there’s a lot of it. Okay, so the reason why he shows up in the red here is that they really want you over 9000 here.
Magdalena W.: Got it, so there’s not enough?
Alan Hopkins: He has … Yes, so we know that if he has LP little a and he has small dense LDL particles, we know that the thing that saves him would be if he had a lot of HDL or good cholesterol to remove all this from the lining of his arteries, right? That’s what HDL’s job is, it removes bad cholesterol from lining of arteries whether it’s LP little a bad cholesterol or it’s small dense, or light and fluffy, that’s what HDL does.
The problem here is his HDL total number is low but even more important to that, the most efficient type of HDL is HDL large and that’s half as much as what he needs and so he’s in real trouble. He’s going to be laying down plaque like crazy.
Magdalena W.: Well, and also just to add on to this for women, we talked about estrogen and the cardiovascular health but also, one of the things that I used to see when I was in private practice was women with low HDL cholesterol, how many problems they had hormonally to produce sex hormones because really, that’s your precursor, that’s your source of producing. Cholesterol is the source producing all your sex hormones.
Alan Hopkins: Yeah, absolutely, yeah. Yeah.
Magdalena W.: That would be like he’s 28, I wouldn’t be surprised if this man also is suffering probably from low testosterone or low DHEA and has like no sex drive and then Viagra is the way of going where actually it’s really the problem is right here.
Alan Hopkins: You know what I love about you? You’re exactly right. He had that exact same problem for that exact reason. Cholesterol is everything when it comes to making our sex hormones so for him, he was low in those markers and this guy needed some serious intervention. I guess my take home point is I’m not here to teach you every single biomarker right now, although I have an opportunity for you to do that if you’re interested, but what I’m here to tell you is that right now we’re not checking the best test to help people, we’re checking test that insurance companies say they will pay for.
We’re not actually intervening early in disease process. We’re waiting for a disease to present itself so there are advanced tests now that can be quite predictive of who’s going to go on to develop problems and that’s what I want to focus on today because I think that you guys can actually be part of a great solution and help people, help lots of people, even if the only thing you do after this is you go and say, “Hey, I heard this weird thing about lipoprotein a and I went on Google and I looked up the NBC’s Biggest Loser trainer. I read the article about him having a heart attack at 51 and I looked at his photo and I just couldn’t believe it and now I’m going to talk to my friends about getting checked.”
If you only did that, you’re going to help people and you potentially could save a person’s life because if a person has LP little a that’s elevated, these are some of the things that need to be done. They need a full laboratory assessment to make sure they don’t have sugar problems, and I’m talking about prediabetes. We want to make sure they don’t have inflammation because we want to try to reverse inflammation if they have chronic inflammation.
We absolutely have to control blood pressure for them. We’ve got to get them to stop smoking if they’re doing it. We’ve got to screen their relatives to see if they also have an LP little a and then we need to know that menopause is going to be a big, big problem for us because when they go through it their LP little a is going to go much higher so we do worry about that.
Inflammation and Hormones
Now I want to talk a little bit about the next thing and sort of bring you along here on inflammation. Inflammation is one of the hottest topics right now in anti-aging medicine and the reason why it’s the hottest topic, it’s really felt like that chronic inflammation is the root cause of many of the chronic diseases and there’s a lot of things that we’re doing that’s causing inflammation in our bodies. If we eat too much sugar, what happens? Well, we store it in our liver as glycogen. When that compartment gets full, we store in our muscles as glycogen. When that gets full, we store in our belly fat and when that belly fat gets full, it releases pro-inflammatory hormones and these pro-inflammatory hormones can actually put you at risk, developing early stroke and heart attack.
Again, our belly fat is the largest endocrine system or our largest endocrine organ in our body and it can produce hormones that are either helpful or harmful. If we measure this and we know hey, I have helpful hormones, that’s great, if they’re harmful, we’ve got to fix that, right? Trans-fats, saturated fats, can also be pro inflammatory. This also can happen when we are deficient with our omega-3s and we have an imbalance there. We’re not eating like we should, we’re not eating whole foods anymore, some people, things are triggering it in their systems, such as dairy and gluten, coffee and so on and the of course, stress is a big thing.
We’re not sleeping like we’re supposed to be and sleep is so restorative, 25% of our life is spent sleeping so it’s so important that we do it well because sleep is when we restore our hormones and we bring everything back into alignment. If we don’t exercise, that could be a source of inflammation. Of course, toxins, infections and so on and in my practice what I see a lot of is weight problems and this thing called insulin resistance syndrome.
An insulin-resistant syndrome is super common and it just means that all these compartments are full, the cells are super unhealthy, and it’s the first thing we see on the road to diabetes so we like to test for it. If you have inflammation, you just need to know you have a higher risk for stroke and heart attack, autoimmune disease and even cancers. When we measure this thing called high sensitivity CRP, if it’s elevated chronically in very high levels I send people in for cancer screening and sometimes we’ll find cancer but most commonly what we find is autoimmune diseases that we just weren’t aware of. People had atypical symptoms, nobody ever checked them before but now these very high levels of inflammatory markers set off the hunt for what the underlying cause was.
Another thing is that there’s an increase in hot flashes with inflammation both in peri-menopausal and menopausal women.
Magdalena W.: You know, I just remembered one more thing about inflammation and hormones. Well, I mean, I think it impacts in every way but the gland’s ability of producing hormones is one thing but also the interesting thing which is I find it so fascinating is that even though you might have adequate hormone levels done by in the blood especially, the problem is that the hormones might not be getting … When a person is inflamed, the cells are inflamed and the cells are not able to uptake that hormone. Even though you have it available and it’s produced, it’s not able to get in through the cell.
To do the work such as having beautiful skin and good mental function and healthy hair, the list goes on, everything the hormones impact which pretty much everything, how we feel and look. That’s another reason to look into inflammation. Needless to say, all the markers that we are talking about here are going to be on the panels that we’re going to show you at the end that we would recommend testing for.
Alan Hopkins: Yeah, the body is a very complex system, right, and unfortunately, it’s not exactly so easy why a person’s hormones may be messed up if they don’t take a comprehensive look. That’s the CRP marker that we’ve talked about. It’s called high sensitivity CRP, great for chronic inflammation. Inflammation is good for us if it’s acute, meaning we bump our elbow on something and it gets swollen up and we want it to heal, there’s an inflammatory process that takes place. What our body does not like is to have chronic inflammation. Inflammation that persists for months and months and months.
All right, now back to the aging well wheel here, the next thing we’re going to look at is actually sugar problems. I got invited by the American Diabetes Association to do lecturing here in Central Texas on the problems with prediabetes and diabetes and what I found is that we’ve got a huge problem here in the United States. I put together a prediabetes reversal program and then I get invited to the Joslin Diabetes Center which was pretty awesome because I got to meet the CEO and he was like, wow, this is a great program. We got to figure out a way to roll this out.
They recognized that the growth of diabetes has been a dramatic thing so if we look at this at the bottom on the X axis is the year, okay, and if you look at the green is the working age people and then if we look at the yellow, that’s the general population so how we’re going to grow over the next couple of decades and then if we look at type 2 diabetes and how it’s taking off. You can see that there’s a huge discordance between our actual growth rate as a general population and the growth rate of diabetes. It’s really reached epidemic proportions and this is an absolute disaster for health care. It’s predicted that, this is by the Center of Disease Control, that one in three people will be diabetic by the year 2050, a couple short decades away. Ninety percent will be overweight or obese by 2050.
If you’re out there struggling with your weight then you’re probably like okay, yeah, this makes sense. If you just sort of walk around and you notice, man, it just seems like there’s so many more people out there struggling with their weight. This is a big problem for us because prediabetes itself, the condition before you ever get into diabetes, you’re going to lose about 50% of your pancreas during the course of prediabetes. When you have no symptoms, half of your pancreas is going to be destroyed.
If we measure the efficiency, how well the pancreas works, you’re going to lose about 80% of the efficiency of your pancreas by the time you’re diagnosed with diabetes. By the time you have diabetes you’re way behind the eight ball and I’m here to tell you the bad news doesn’t end there, there’s also an increased risk for cancer when you’re in prediabetes and also an increased risk for early stroke and heart attack. Our body does not like to have high sugar levels so when we look at sugar levels, the very first thing we start to see for most people is insulin resistance. This is just a sign that all the compartments that we talked about, your liver and your muscle and your belly fat are completely full and now insulin’s out there in the bloodstream and it can’t push anymore sugar in to these cells that are super unhealthy. This leads to all kinds of problems. Again, the ultimate end product is dying from a stroke or heart attack.
Heart attack is the number one killer here in the US. Stroke followed shortly thereafter. At the end of the day, all these things work together based on sugar problems so when you get overweight, you’ll get the small dense LDL because of insulin resistance, your HDL will become lower, you become much more likely to form a blood clot which means that if you have an LPA in addition to this problem, you’re in real trouble.
Of course, we all struggle with weight. That’s the story there but if we look at testing, these are the tests that are commonly offered for this issue. The first one you can get it at your doctor’s office and you should get one done every year and that’s a glucose. The other one is a three-month sugar measurement called the A1C, but if we’re talking about aging, I want an advanced test. I want to know even before my sugar starts giving me problems, I want to know am I on the road to having a problem? The best test for this is looking at your fasting insulin. The lower your fasting insulin level is, the better the situation is for most people, all right. That’s assuming you don’t have diabetes already and you can’t make any insulin because that’s what happens. If you lose half your pancreas and you lose just a little bit more, your blood sugars go from 110 all the way up to 3 or 400 literally overnight because enough of your pancreas has died and you just can’t make enough insulin. The initial response of the body to stress with carbs is to produce tons of insulin, so that’s the first thing we’re going to see is called insulin resistance syndrome.
The healthiest people on my practice have insulin levels less than two so I consider that to be optimal. The higher it goes, the higher the problem is. Glucose, if you want to know what I think a perfect number is, it would be between 70 and 85. We all tend to creep a little bit higher as we get older. The definitions from the American Diabetes Association for prediabetes are glucoses between 100 to 125, that’s consistent with prediabetes. If your glucose is above 125, that’s more likely diabetes.
Now nobody, I’m just talking from a doctor’s standpoint, nobody really diagnoses diabetes based on one single fasting glucose. They tend to also order the hemoglobin A1C because on that particular day, maybe you’re in a car wreck or some sort of stressful event just prior to getting to your appointment and you released a bunch of cortisol which caused your sugar to go up and confused us. We do this A1C measurement too. This is more an approximation of the three months of daily sugars.
Much more reliable to make the diagnosis of diabetes on. If you’re above 6.5%, we call that diabetes, if you’re between 5.7 and 6.4, we call that prediabetes. Less than 5.7 is considered normal however, in anti-aging, we like even less so less than 5.4% is considered optimal. If you think about sugar as a continuum over time and you’re able to intercept it in the earliest stages, you want to be looking more at insulin and unfortunately, doctors really aren’t checking that like I believe they should. I believe everyone should get at least an insulin, a glucose and an A1C checked every single year to monitor for this, particularly since I’ve already told you that 86 million of you already have prediabetes and 90’% of people have no symptoms.
The symptoms of diabetes don’t really occur until your blood sugar goes above 250 for most people and that’s because your kidney is signaled at 250 to start releasing water and so you’ll start shutting off water which will cause you to urinate all the time and then cause you to be super thirsty, right? I wanted to talk a little bit about some of the symptoms. I’m going to show you that in just a minute.
Insulin resistance is probably one of the number one problems I see with weight loss. This is especially common after menopause, so if you’re out there and you’re putting on weight and stuff and you’ve never had your fasting insulin checked, you probably should check it. The blood test will show the fasting insulin that’s high and you may not have yet developed the other findings of sugar problems which are prediabetes and diabetes so your blood sugars may be okay and your A1C level’s may be okay but your insulin is through the roof. If you just know that if you could improve your blood sugar control, that’s going to improve your symptoms, such as hot flushes, that may be somewhat motivational. There are real risks besides symptoms too. We’re talking about end of life risk as you have increased risk for cancers and strokes and heart attacks as you go through the sugar continuum. The worse that your sugars go or the higher they go, the higher your risk goes. Also, insulin resistance syndrome is the number one cause of PCOS.
If you have polycystic ovary syndrome, you have trouble with infertility, you’re missing your periods, you’re having acne, irritability, mood changes, those kind of things, look at your fasting insulin. It, along with your androgens or testosterone and so on, will be abnormal. Just simply fixing that is going to really help you. It help normalize everything. I touched a little bit on this a second ago. As your blood sugar goes higher and higher, you can get thirsty, you can urinate all the time, you get blurry vision from the sugar binding to the proteins in the back of your eye there. You can experience fatigue, extreme fatigue.
If your sugar is low, you can have the opposite things like being anxious, and shaky, and sweaty, moody, and lack of focus that can happen for some people when their blood sugars were low. Premenopausal women, I see a lot of PCOS or polycystic ovary syndrome, really high levels of fasting insulin along with the acne and the irritability, problems with fertility, those kinds of things. Then, of course, the trouble with the weight loss is huge whether you’re premenopausal or postmenopausal if you have really high insulin levels. Postmenopausal women tend to have increase hot flushes, increase belly fat, and that’s not a good thing.
You don’t want to begin to look like grandma before it’s time. That’s really what happens. As we go through menopause, we start to become like our grandma. We start looking like grandpa. Grandma and grandpa look very similar at the age of 70. My objective for you guys here is, number one, education. That’s the opportunity that we have that’s a little bit different. Being able to order labs yourself, you can get it done through lots of different platforms. I encourage you to also get educated too. We do have a special offer for you through the Hormone Balance website for this community.
Then, at this point, I’ll turn over to you, Magdalena W. to go through the different things that you wanted us to put together for your community and talk about at what you see is value.
Order Lab Panels – Offer for the Hormones Balance community
Magdalena W.: Yeah, let’s do that. Like Dr. Alan mentioned, the URL is go.yourlabwork.com/hormonesbalancelabs. We are going to make the URL available in all different places. Just before I show you the labs, just want to share that it’s a really simple ordering process. You order them online with the link down below here. You go to the local quest lab, which has got over 4,000 locations throughout the country. Then, you get the results online within 48 hours, really as simple as that, just absolutely wonderful. No need to see a doctor, no need to argue why you want to have those labs done. We always get a lot of questions of what about us Canadians, what about us in the UK. We can’t help you with this.
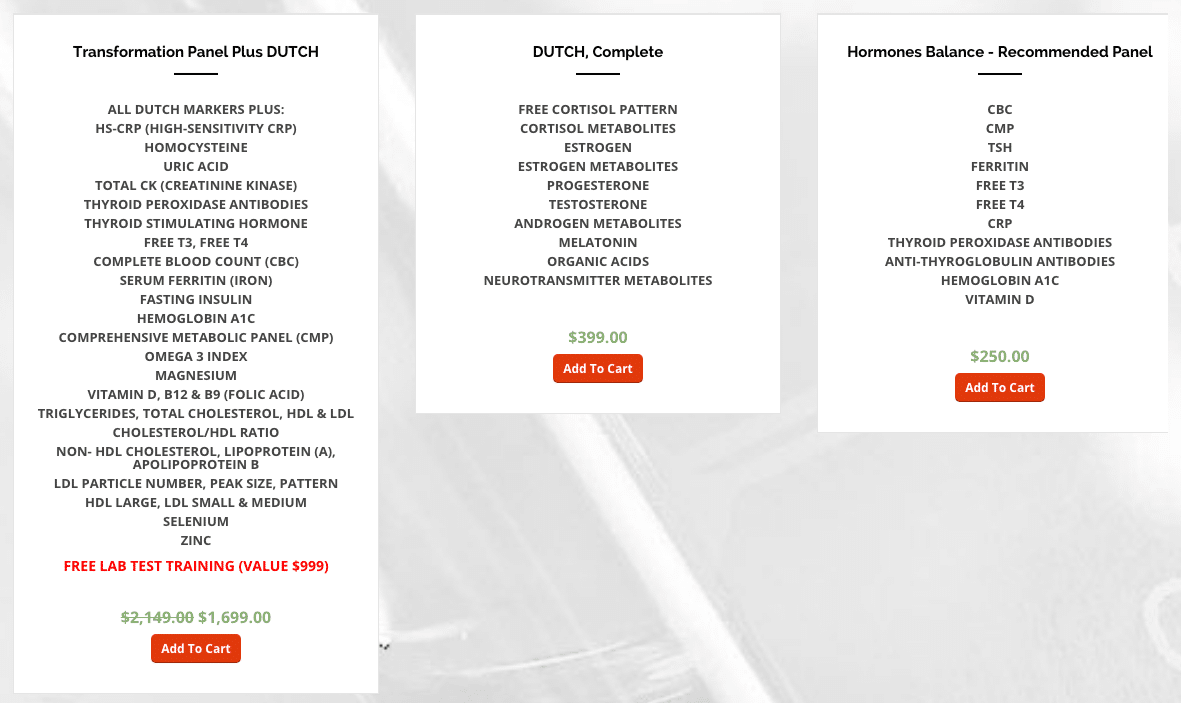
What you can do is use all this education and to find a private doctor and then work with him or her. All right, here are the three packages that we have for you. It’s the transformation panel plus DUTCH. The transformation panel would have a lot of the markers Dr. Alan mentioned today. You saw everything from the DUTCH’s included here, plus we’ve got the CRP, the homocysteine, uric acid, and the list goes on. I’m not going to read through everything here. You can pause the video and just look at that. We have an option for you for … Before I mention that, the package here is $1,699. What this package does include is education from Dr. Alan on every one of these markers. What they mean, what are the functional ranges and more importantly how to mitigate. The other smart thing they have done, which is I can completely appreciate those … Is that what you call it, cheat sheets?
Alan Hopkins: Yeah, yeah, absolutely cheat sheets. I’ll talk about those in a minute. We have cheat sheets for people to try and make it easier for them.
Magdalena W.: My cheat sheets for food and nutrition are also so popular because it’s something you can … I know you laminate them and all that, and you could have them just hanging on your office wall if you’re a practitioner or having it in the kitchen, your office. It’s just a quick referral without having to do tons hours of research. The internet can be great, but it can also be a problem because you get a lot of contradictory information. The second panel is DUTCH alone. That’s the DUTCH complete that we’re offering here. It gives you the full cortisol panel throughout the day, and then also shows us the cortisol metabolites, estrogen, and estrogen metabolites, progesterone and ill factor progesterone metabolites, testosterone metabolites.
Everything is actually where the metabolites, but also melatonin, organic acids which are really beneficial in understanding on how your metabolism is basically working. Powerful neurotransmitters which can indicate a lot of mood stuff going on, including depression, anxiety, addictions, obsessive behavior, that kind of stuff can all come out from here. That panel is $399. Then, we have the hormones balance recommended panel, which is the basic stuff. If you feel like maybe panel one, panel two is not for you, then the panel three gives you the basics of the CBC. That’s your complete metabolic panel with a TSH so that your thyroid marker for ferritin, that’s your iron storage in the liver, free T3, free T4, and the list goes on.
I don’t need to read that. This is a great starting point, especially if you have already done a lot of things in the past. We basically repackage the panels into three options here. If you feel like maybe you want to just pick and choose what you want, there is always an option of that. I love this website for that. You could just basically click on what would you like to order, and then go and add it to cart, and then check it out. Everything that Dr. Alan has covered is all in here. I didn’t even see that. We have even exposure. This is heavy metal testing here, right?
Alan Hopkins: Yes.
Magdalena W.: Yeah, that’s awesome. Well, you have even genetic testing, okay.
Magdalena W.: Specific markers.
Alan Hopkins: Yeah, we’re adding things as people are coming to this thing, it is what we’d like to see.
Magdalena W.: I love the interface, it’s just so super simple and just absolutely lovely. That’s that and the URL is going to be below this video. Would you like to share with us more about the education piece because I know a lot of people are going to be super interested in that?
Education included with the Transformation Panel
Alan Hopkins: Yeah, for sure. Let me get there here, see if I can get to the education piece. The idea here was that we were going to do this a little bit different for your community because they were already fairly well-educated and they’re very interested. Can you see this here?
Magdalena W.: Yeah.
Alan Hopkins: Okay. The idea here is that if they decide to purchase the large package, we want to give them a ton of great information. What is this information? Why do a deep dive lab training on every single one of the pillars of health that we offer? We talk about hormones. We’re going to talk about the cholesterol. We’re going to talk about insulin dynamics. We’re going to talk about inflammation and nutrients. We’re going to go through each individual test and give in-depth explanations on what they’re actually measuring and what the optimal levels are, and really how you can get there. I also have PowerPoint lecture download.
Maybe if you’re a health coach, you’d really like this because you can use this in actual pieces to put together yourself and some evidence-based tools that you can use yourself either as a client or for somebody else. An example that comes to mind is sleep. I mentioned before, we were missing obstructive sleep apnea. It’s fairly easy to pick up if we just look for it. One of the things we look at is a very low, lower than expected, morning cortisol level. Whether we see that on a DUTCH or we see that on an a.m. serum cortisol test, if we see that, you just download my sleep tools. There’s two worksheets with 10 questions each.
If you fail one or both of those, either one, all you had to do is take it into a sleep doctor. Your insurance will then cover it, the sleep test based upon the fact that you’ve failed these things. Because you’re put out by the American Sleep Academy, the people that actually run the sleep specialty. These things are really evidence-based and evidence-led. Or if you fail that, you just take it in, you get the test done. Guess what? If it gets diagnosed and properly treated, all of a sudden, we get the weight loss, we get the hormones working better, we get the cholesterol going down. We can reverse prediabetes and sugar problems with that and give the person energy, a lot of little tools in there that are meant to really help people in a meaningful way.
In addition to all the explanations, we want to give explanation but we also want to give real life things that my health coaches actually use with my patients in my practice. This offer includes these blood tests plus the DUTCH. It was important for us to add on the DUTCH here for Magdalena. We decided we throw that in. You might want to know exactly what’s offered. For hormones, it’s going to be a little bit different here because we’re going to give you the DUTCH, we’re going to give you the thyroid test. That includes the TSH, the active thyroid hormone called free T3 and then free T4. Then, we’re going to also check your antibodies.
Because if your antibodies are positive, then that’s going to mean that you have Hashimoto’s disease. It’s very important to know about that early on. We want to hope that your antibodies will be normal. The sex hormones are going to be provided by the DUTCH. I won’t go into that anymore. The metabolism, of course, if we’re going to look at the continuum of blood sugar problems, we definitely want to look at that fasting insulin. Because remember, that’s the first thing I said, is it going to be super high on the road to diabetes? We’re going to intercept that early. We also want to look at your glucose and your A1C.
It’s very important for us when we’re looking at these tests to look at a comprehensive metabolic panel looking at your liver function, your kidney function, making sure everything is normal there, and measuring electrolytes and protein stores. We also do a complete blood count where we’re going to look at for any anemia or leukemia. I remember I had a six-year-old girl brought to me in the Emergency Room by her parents who said, “She just not as energetic. We just want to get her checked.” I did some testing on her and I found that her white blood cell count, which is part of the CBC, was 50,000. That should be less than 12. That poor little girl had leukemia.
A blood test is looking at your bone marrows, really important to do at least annually she get a CBC done. Anyway, we included that. Cholesterol, you know me based on our short time together, you already know that I’m going to recommend the advance cholesterol panel. I want you guys to have the best test available, not just the standard test. This, of course, test is never covered by insurance. It’s a hardly ever done. It’s so important to get it checked and make sure you don’t have that lipoprotein A, because you’re going to find out on that test. Also inflammation, not only are we going to look at that high sensitivity CRP which is a great inflammatory marker, but we’re also going to screen you to see if you have high homocysteine.
High homocysteine can be fixed quite naturally. It would be nice to know about it now as opposed to waiting until you have some cognitive issues. Again, we’re not certain that treating it early is going to be 100% protective. Everyone agrees and is on the same page that the treatment is natural and it’s easy, and it should be done. Also, we want to look at breakdown products to your muscle called CK, just to make sure you’re not over exercising or make sure that you don’t have an autoimmune attack on your muscles. We’re looking at the CK muscle enzyme. Then finally, uric acid, I love to check for this because there’s such a strong association with high uric acid in prediabetes.
We know there are so many people out there with prediabetes. The thing that I learned the other day also is that uric acid levels can be quite high if you’re on a ketogenic diet. If you have high levels of uric acid, it put you at risk for developing gout. Gout is a disease that I see people in the ER for. They usually come in with severe pain in their joint, usually the base of their first toe or maybe their elbow or knee. They just feel like cutting it off. I’d rather to know if somebody’s at risk for this and to be able to show you how you can lower this very naturally. We have a downloadable sheet if you have high levels of uric acid for you to download yourself.
Nutrients, we talked at length about these nutrients. I also threw in zinc and selenium. These are also very important nutrients that we test in addition to everything else that you can read there. The idea here is to do a very comprehensive approach in your laboratory testing. I want to provide you with a way to look at these things too so you can take all the questions to your provider with some really good information. Again, this is evidence-led information. I’m going to provide you with something called optimal valued cheat sheets. If you’re ever wondering what it’s like to see an anti-aging doctor or maybe you see a functional medicine doctor, one of the things that you’ll learn if you’ve seen a bunch of them is that everybody has a little bit different way of doing things.
Well, most of us agree on what optimal ranges are. Conventional doctors don’t really understand optimal ranges because they’re not really treating for optimal, they’re just treating disease. Before I did all my training, advance training, I just knew it is normal or not normal. Now I know this thing called optimal. These cheat sheets were formulated to number one tell you what the biomarker was, give you a brief description of the biomarker, what it’s actually measuring. Then, in that gray thing that you can see there, that’s the optimal levels where we would like to see you at least in my practice. Then to the right is everything that you can do naturally to improve each biomarker.
Some of them, we have a lot of things you can do naturally. Others, there’s a few things that you can do. These biomarker cheat sheets have become extremely popular because people love to look at their own lab work with these things next to it and then they circle their issues or having trouble. Then, they work with their provider whoever is helping them to come up with an overall plan for their health. By looking at everything in a comprehensive way, we can now hone down on your specific issues. All right, so if I’m going to do this for your group, I thought it would be really good to do a group live lab review webinar.
If we had enough people go and get this comprehensive testing done, they would probably benefit for me coming on and answering questions and going through an example of a comprehensive test and talking about each one of the biomarkers and what optimal is and how you get there. It just would reinforce that learning process in the brain and maybe pick out a few things that people weren’t thinking about. We also thought it would be good for a question and answer session to do. Now, when it comes to DUTCH, Magdalena, we had talked about this. We do have a specialist, an OB-GYN doctor that I worked with who knows DUTCH very, very well.
He also is willing to help us with this. I could probably go ahead and get him to come on this live lab review too. I, more importantly, want to give you guys access to him via telemedicine. I’m working with him and we’ll work with Magdalena, so that each one of you that has had the DUTCH specialty testing done, which is very comprehensive, has the opportunity if you want to, to have a private telemedicine consultation with him.
Magdalena W.: That’s so important. I have worked and refer its people to Dr. Shawn Tassone for a couple of years now. He is not just very knowledgeable but very empathetic and really, really sweet practitioner who women just absolutely love. This is great. The links are below. If you guys have any questions, as always, [email protected] is the email to send in your questions. If there’s something we don’t know, we will definitely reach out to Dr. Alan and get things clarified. Is there anything else that you would like to add just to close this off?
Alan Hopkins: Yeah. I just wanted to thank you for the opportunity to be able to come to your group and talk about ways that we can help optimize people. People sometimes do get confused, and I do want to make it just clear. I’m not anybody’s doctor. This actually isn’t a medical practice. This is a non-medical practice. As part of what our mission is, our mission to up level everyone’s IQ on lab testing because we want that person to be able to go into their visit with their provider with a lot of really good information, stuff that’s backed by research, natural ways that maybe the conventional doctors aren’t necessarily thinking about and force that doctor to actually sit down and go through each one of these questions based on real data, which is your lab work. We’re very passionate about that and adding that extra value add-on. If we can’t add on Dr. Shawn Tassone to review the DUTCH testing, that’s an awesome, awesome thing for us to do.
Magdalena W.: Yeah. This is fantastic. I am so glad that you’ve decided to go in this direction and create this practice because this really has been a dream come true to address so many emails that we get on the daily basis asking us about testing. Two, three years ago, I did a Facebook Live on what to test for and is one of the most popular videos that we have, most watched. I couldn’t really help. My answer to people was go and find it with doctor, go and find a functional practitioner who will order these labs for you. A lot of it gets resolved. I’m so happy that I have found you and this is phenomenal. I have also met a few coaches who have gone through your education program and they read about it.
Alan Hopkins: Great. Yeah, great. That’s awesome.
Magdalena W.: Because I think you’re important, okay. Fantastic. We’re going to also get this video transcribed. If you don’t want to watch this, you can also just look at the text. I’m more of a reader than a watcher on the video. Want to give you a couple of options of how you want to consume the content. As you know, you can order the test on the URL. It’s going to be below this video. Thank you so much, Dr. Alan.
Alan Hopkins: Yeah, thanks so much for having me. I really appreciate being on. Okay, all right.
Please note that this is a sponsored post, meaning I do receive a small percentage of sales, but all opinions are my own.
Thanks a heap for all the info! Do you have any idea where one would find self-request laboratories offering these tests in Queensland, Australia?
Hi Annette, as far as we know there are no services like this in Australia. The closest thing would be requesting labs from an naturopathic doctor and paying privately, ~ Jeanne HB Team.
Thank you so much for the informative video.
Please send the information regarding ordering in Canada.
Thank you,
Lori
Hi Lori, Unfortunately there are no services like this in Canada as far as we know. The closest thing would be requesting labs from an naturopathic doctor and paying privately, ~ Jeanne HB Team.
Thank you Magdalena for bringing Dr. Alan. Two questions:
-For those of us already getting the labs, does Dr. Alan have available ONLY the ‘cheat sheets’ with his optimal ranges for test results?
-Will you put together a program for those of us senior to your age that focuses on special needs/issues for healthy post-menopausal women?
HI Lisbeth, yes, you can reach out to Dr. Alan’s customer service and request to purchase the “Cheat Sheets” they have available for blood work. Here is the link: https://yourlabwork.com/hormonesbalance/
Without knowing a health history, it would be impossible to determine which labs anyone needs. Magdalena gets the Transformation Panel Plus Dutch once a year. I hope this helps! ~ Jeanne HB Team
Actually my comment is about an article you wrote on infrared saunas. You posted a list of places where one could try a sauna for themselves. Somehow I lost that content and would appreciate being sent that list thank you.
I Will tell you that this platform with Dr. Alan is fantastic. I hope to use this in the future
Hi Michele, here is the article Magdalena wrote about the healing benefits of infared saunas: https://hormonesbalance.com/articles/adrenals-articles/healing-benefits-infrared-saunas/ Magdalena first tried one at a yoga studio ~ Jeanne HB Team
Very useful conversation! Thank you so much for posting this useful article with us! I am constantly asked this question: What Is The Best Way To Test Your Hormones? Regarding the various methods available for hormone testing. Unfortunately, there’s not a simple answer because each of the methods has unique pros and cons. The question is compounded by the fact that doctors and researchers have differing opinions on which testing method is the best. Making the matter even more complex, laboratory companies with vested interests also muddy the waters by presenting biased evidence showing that their way is the best way
Stem cells treatment
Thank you for sharing your thoughts on this article Meredith
~Deanna HB Team
I know my insurance does cover some of these labs and that Quest is a preferred provider (as I work for my insurance company). My question is… will I get the required payment documentation from Quest to self submit to my insurance if I order from this website?
I also know that Quest offers deep discounts as an “contracted” provider so if I were to have these tests ordered by a physician would I still be able to participate in the lab review with Dr. Hopkins and get the cheat sheets, free lab test training, etc?
And… since the DUTCH is a urine sample over time is that done through Quest as well or is that a separate thing? It was stated in the interview that it was a kit that is sent to you home and sent back to the lab.
So many questions here. Lol
Hi Karen, I checked the FAQ and found this answer for you:
“We do not take insurance or participate in Medicare, Medicaid or other governmental or state programs. If you have a Health Savings Account or a Flexible Spending Account, we can provide an itemized receipt after your blood draw. Contact us [email protected] once your results come in and we will issue an itemized receipt”
No, that offer was for purchases made through Yourlabwork.com.
You will need to contact Quest to find out about their Dutch test, it could very well be the same test:)
~ Jeanne HB Team
Hello
I am following Magdalena’s protocols in every aspect of my life with diet and lifestyle down to a science and planning on getting the transformation panel and the Dutch, but before I do, how would I need to prepare for the tests to get accurate results if I am supplementing with progesterone, DHEA, and some estriol to deal with severe symptoms that I cannot get under control yet even with all the protocols I have incorporated in my diet and lifestyle? I’d like to get an accurate reading as to exactly how my body is working without any influence of biodentical hormones, but I am still just too symptomatic .
Thanks in advance
Hi Teresa, We recommend working with a skilled practitioner who has years of experience with bioidentical hormones as Estrogens and DHEA/testosterone can be tricky and if you do not break them down properly, this can lead to worsening symptoms and even development of hormonal cancers, fibroids, endometriosis, and facial hair. If you need help locating one in your area, here is a good tool
https://www.functionalmedicine.org/practitioner_search.aspx?id=117
I hope this helps!
~ Jeanne HB Team
This is wonderful news but i cant pay for all those blood test. Im on medicare just had TSH Reflex Free test done, it reads 1.01 uU/ML
still feel like a zombie. My mother had her thyroid taken out years.
ago. I know the test are needed. Just will have to live like a zombie
the weakness is really bad spend most of my time in bed.
Feeling like a zombie,
TY,
Diane Gifford
Hi Diane, It is very challenging when we don’t feel well. Here is a link to Magdalena’s blog https://hormonesbalance.com. There are free recipes, recommendations and resources. We hope you check it out. ~HB Team
Is it better to test during one point in your cycle rather than another to get the clearest results? I was going to order the DUTCH complete and the Hormones Balance – recommended panel. I always feel the worst in the second half of my cycle. I haven’t had any previous testing done but have started seed cycling and making dietary changes.
Hi Erin,
Good question. There is a certain window (after ovulating) that is best for testing. When you get the test, there are instructions/support ~HB Team
[…] My estrogen dominance was diagnosed based on a simple blood test called the 2:16 Hydroxyestrone Ratio (more details below). You can also get it tested through saliva and get a better view of the different estrogens, progesterone and their relationship to each other. I share more about saliva hormone panel testing here. […]
[…] Do you suspect you have a thyroid condition? Don’t worry, you can bypass a doctor so you don’t have to convince them what test to order and avoid paying expensive appointment fees. If you’d like to get tested it’s pretty simple, just click right here. […]
[…] 3. Metabolites: When estrone metabolites called 2:16 hydroxy-estrone get broken down unfavorably towards the “dirty” metabolite – 16 hydroxy-estrone (that tends to be highly estrogenic and act on the estrogen receptor). I like to use DUTCH urine test to check these metabolites. You can read more about which lab tests to order here. […]
I agree 200% on the PPT slides. Hormones are part of glands. I live in Los Angeles, California. I am 52 years old. I live Keto….I avoid red meat and dairy (not whole eggs). I have a Natural Medicine On-Line……Stress is the one that has caused a lot of problems. I am not working and I have an HMO/Medicaid Plan…..Loma Linda is located in here in Orange County, which is very far for me. I live in the Suburbs of L.A.. I know I have hormone issues, but I need to see someone here….is there anyone that you can recommend…..if your office is here in L.A…that is great. If not, please refer me to several hormone Dr’s (no student Endocrinologists) The Endo’s out here do not know anything……I know more than them.
Hi Robert,
Please send an email to [email protected] and the team will send you some resources. ~HB Team
Hi, this is a question for Dr. Alan. I subscribed to watch his webinar with Dr. V. He is offering us a discount on lab work. However, I am not sure if I have cancer or not. I had some symptoms in my breast that went away with some changes to my lifestyle, but I haven’t been willing to do a conventional test for that matter. My question is, what is the best test, among the tests he is offering, to determine that I don’t have it? Please let me know ur answer. Thanks a lot,
Thank you for reaching out in email as well. We sent some resources your way! HB Support
Hi, is it your health problem or which of your family members? First you need to understand acquired or inherited ataxia. It is better to conduct a quality examination and choose the right treatment method. My aunt, undergo treatment at the clinic https://www.startstemcells.com/ startstemcells hospital , which was advised by our doctor. Here, doctors have more modern treatment approaches that give a good result. You can also come here for help. The site has all the necessary information that is useful to you. It employs professionals who have rich experience.
[…] Because our ability to heal slows down as we age, that irritated skin may stay that way longer, contributing to equally irritated emotions! There are now self-order lab tests you can get, if you’re not sure what your hormone status is. Here’s an article that covers how you can get access to these lab panels. […]
Dr Alan:
My question has to do with Current CoVid I work in retail at the mall and have been exposed to both fragrance and lots of chemicals from skincare product although my biggest concern is I’m in the midst of getting a work accommodation petition granted through a third party company and when ai faxes the info with the request of telling my workplace to stop scanning my forehead with a forehead laser gun and redirect it to my wrist after doing my own research and found out from New Jersey study from a group of drs who claim that those laser guns affect my pineal gland and damaged my retina!! My OBGYN refused to help!! Your professional advised is greatly appreciated for my livelihood is in the balance,
I’m a very concerned patient!!
Sincerely,
Marisol G
I am interested in ordering the Dutch panel test. I have been on birth control pill for over twenty years. After accepting for too long the treatment of amenorrhea with birth control I’m desiring to understand what the root cause is. Is it thus advisable to come off birth control before taking the hormone panel?